


You Are A Lab Rat
How Medicine Makes Patients Unwilling Test Subjects

No man has the right to disease another on any pretext. If vaccination was prophylactic against small-pox, its infliction would nevertheless be wrong and without justification...[1]
— Alexander Wilder, MD, Professor of Physiology, United States Medical College, New York, editor of the N. Y. Medical Times

Audio in this article was created using ElevenLabs. With ElevenLabs, you can generate high-quality speech in any voice, style, and language. Their AI voice generator delivers incredible human-like audio that will blow your mind. Please consider clicking on the affiliate link to check them out. https://try.elevenlabs.io/1bv65kr0oz9w
Imagine waking up to find yourself trapped in a cage—an invisible one—yet confining all the same. Unbeknownst to you, you've been enlisted in an experiment you never consented to, your life entwined with forces beyond your control. You might assume that any drug or vaccine given to you has been rigorously studied, designed only to heal, never to harm. But that assumption, as you’re about to discover, could be fatally mistaken.
The medical establishment sees you as part of an unending experiment, a subject for trial in an array of medications and vaccines—without ever being fully informed of the potential dangers. You likely trust that these products are meticulously tested, believing corporations and governments would never risk your well-being. But history tells a different story. Remember Thalidomide? Vioxx? Rezulin? Avandia? Baycol? These drugs are stark reminders that blind trust can come at a devastating cost. Yet, these pharmaceutical disasters and their victims are mostly forgotten.
Thalidomide – Used to treat morning sickness in pregnant women, it caused severe birth defects in over 10,000 babies globally, leading to limb deformities.[2]
Vioxx (Rofecoxib) – A non-steroidal anti-inflammatory drug (NSAID) for arthritis and pain relief, increased the risk of heart attacks and strokes, leading to an estimated 88,000 to 140,000 cardiovascular events in the U.S. alone.[3]
Rezulin (Troglitazone) – Used as a diabetes treatment, it resulted in 63 confirmed deaths from liver failure and thousands of liver injuries.[4]
Avandia (Rosiglitazone) – Used to treat type 2 diabetes, Avandia may have caused as many as 100,000 heart attacks, strokes, deaths, and cases of heart failure since it came on the market in 1999.[5]
Baycol (Cerivastatin) - A cholesterol-lowering drug withdrawn in 2001 due to its link with rhabdomyolysis, a condition that can lead to kidney failure and death. Baycol was withdrawn from the market because of 52 deaths attributed to drug-related rhabdomyolysis that led to kidney failure.[6]
Over the past five decades, studies have revealed startling death tolls linked to adverse drug reactions (ADRs) and other drug-related complications in hospitals. Conservative estimates suggest 60,000 to 140,000 ADR-related deaths annually, though this likely underrepresents the full scale, given a lack of data on outpatient and long-term care populations. Research highlights an estimated 128,000 annual ADR deaths among hospitalized patients, placing ADRs as a top cause of death, comparable to stroke. Studies estimating up to 400,000 preventable hospital deaths annually due to medical errors position these errors as potentially the third leading cause of death in the U.S.
We can conjecture the range of 60,000 to 140,000 ADR [Adverse Drug Reaction] deaths to be probably extremely conservative since we have no data measuring drug-induced deaths in the ambulatory and extended care populations.[7] – Journal of the American Medical Association, August 19, 1974
Appropriateness of the model may be judged by comparing the results of this analysis with findings from previous reports of drug-related morbidity and mortality. Our estimates appear to be in line with those of other reports. The estimated number of deaths owing to DRPs [Drug Related Problems] in this analysis ranged from 79,159 to 198,815 deaths.[8] – Journal of Managed Care Pharmacy, 1996
2.7 million hospitalized Americans each year have experienced a serious adverse reaction. Of all hospitalized patients, 0.32 percent died to ADRs [Adverse Drug Reactions], which means that an estimated 128,000 hospitalized patients died annually, matching stroke as the 4th leading cause of death. Deaths and serious reactions outside of hospitals would significantly increase the totals.[9] – The Journal of Law, Medicine & Ethics, October 2013
It does not matter whether the deaths of 100,000, 200,000 or 400,000 Americans each year are associated with PAEs [Patient Adverse Events] in hospitals. Any of the estimates demands assertive action on the part of providers, legislators, and people who will one day become patients. Yet, the action and progress on patient safety is frustratingly slow; however, one must hope that the present, evidence-based estimate of 400,000+ deaths per year will foster an outcry for overdue changes and increased vigilance in medical care to address the problem of harm to patients who come to a hospital seeking only to be healed.[10] – Journal of Patient Safety, September 2013
A literature review by James estimated preventable adverse events using a weighted analysis and described an incidence range of 210,000-400,000 deaths a year associated with medical errors among hospital patients. We calculated a mean rate of death from medical error of 251,454 a year using the studies reported since the 1999 IOM report and extrapolating to the total number of US hospital admissions in 2013. We believe this understates the true incidence of death due to medical error because the studies cited rely on errors extractable in documented health records and include only inpatient deaths. Although the assumptions made in extrapolating study data to the broader US population may limit the accuracy of our figure, the absence of national data highlights the need for systematic measurement of the problem. Comparing our estimate to CDC rankings suggests that medical error is the third most common cause of death in the US.[11] – British Medical Journal, May 2016
Yet, despite overwhelming evidence, governments and the medical establishment seldom bring these injuries and fatalities to the forefront. The staggering death tolls remain largely unaddressed, with scant attention given to the critical need for reform and the systemic failures that place countless patients at risk each year. The Centers for Disease Control (CDC) doesn’t even keep track of drug deaths or medical errors.
But what about vaccines? Certainly, those are tested in a lab and are determined to be “safe and effective” before they are used on humans. Yet, children of mothers in prison, the mentally challenged, and the poor in other countries were experimented on by vaccinators. This was admitted in a 2018 testimony of Stanley Plotkin, the Godfather of vaccines, in the State of Michigan in the Circuit Court for the County of Oakland Family Division in the case of Lori Ann Schmitt vs. Michael Schmitt Case No.: 2015-831539-DM.[12] [Actually audio recording]
Q Have you ever used orphans to study an experimental vaccine?
A Yes.Q Have you ever used the mentally handicapped to study an experimental vaccine?
A I don't recollect ever doing studies in mentally handicapped individuals. At the time in the 1960s, it was not an uncommon practice.Q So you're saying -- I'm not clear on your answer. I'm sorry. Have you ever used mentally handicapped to study an experimental vaccine?
A What I'm saying is I don't recall specifically having done that, but that in the 1960s, it was not unusual to do that. And I wouldn't deny that I may have done so....
Q Have you ever expressed that it's better to perform experiments on those less likely to be able to contribute to society, such as children with handicap, than with children without or adults without handicaps?
A I don't remember specifically, but it's possible. And, again, I repeat that in the 1960s, that was more or less common practice. I've since changed my mind. But those were, that was a long time ago....
Q I'm going to hand you what's been marked as Exhibit 43. Do you recognize this letter you wrote to the editor?
A Yes.Q Did you write this letter?
A Yes.Q Is one of the things you wrote: The question is whether we are to have experiments performed on fully functioning adults and on children who are potentially contributors to society or to perform initial studies in children and adults who are human in form but not in social potential?
A Yes.Q It may be objected that this question implies a Nazi philosophy, but I do not think that it is difficult to distinguish nonfunctioning persons from members of ethnic, racial, economic, or other groups.
A Mm-hmm.Q Have you ever used babies of mothers in prison to study an experimental vaccine?
A Yes.Q Have you ever used individuals under colonial rule to study an experimental vaccine?
A Yes.Q Did you do so in the Belgian Congo?
A Yes.Q Did that experiment involve almost a million people?
A Well -- well, all right, yes.
It wasn’t only the mentally handicapped, babies of mothers in prison, and the million or more poor in other countries, but ultimately, they needed to do their experiments on the general public.
In 1949, Alexander Langmuir, MD, known today as “the father of infectious disease epidemiology,” created the epidemiology section of what became the CDC. He also headed the Polio Surveillance Unit, which was started in 1955.
In the fall of 1955, the year the Salk polio vaccine was released, Dr. Langmuir had predicted that by 1957, there would be fewer than 100 cases of paralytic polio in the United States. Given the nearly 6,000 reported cases of paralytic polio, the Salk vaccine fell, to put it mildly, significantly short of the lofty expectations. In 1959, one-third (33%) of paralytic polio cases were in those who had one or more doses of the Salk vaccine. Over 16% had three or more doses of the vaccine. According to Dr. Ratner:
Four years and 300 million doses of Salk vaccine later, we had in 1959 approximately 6,000 cases of paralytic polio, 1,000 of which were in persons who had received three and more shots of Salk vaccine.[13]
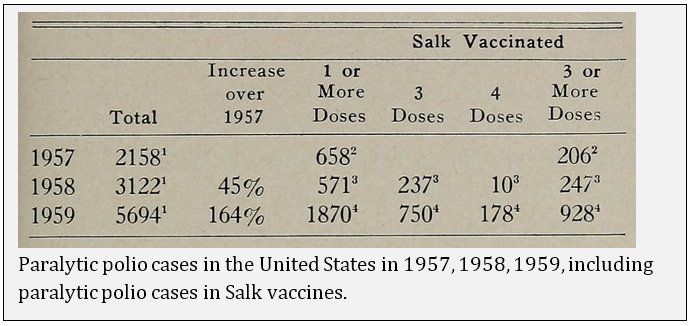
Dr. Langmuir was right when he said the disastrous figures of 1959 were “sobering.” Dr. Sabin said the number of cases in 1960 was less than in 1959, but 23% occurred in persons with three or more doses of the Salk vaccine. Not only was the vaccine failing, but it was causing polio and, in some cases, resulting in death.
Mass vaccination with the Salk product started in April, 1955, and by April 26, there were reports of paralytic polio among vaccinated children, with deaths occurring in Idaho and California. Then came cases of polio among family members of vaccinated children. Live virus was discovered in the supposedly killed vaccine, although it had been produced by the Salk procedure.[14]
The long-forgotten Cutter manufacturing disaster injured many and killed some.
In the end, at least 220,000 people were infected with live polio virus contained in Cutter’s vaccine; 70,000 developed muscle weakness, 164 were severely paralyzed, 10 were killed. Seventy five percent of Cutter’s victims were paralyzed for the rest of their lives.[15]
While the vaccine was being rolled out, the definition of a polio case quietly shifted. The practice among doctors before 1954 was to diagnose all patients who experienced even short-term paralysis (24 hours) with “polio.” In 1955, when the Salk vaccine was released, the diagnostic criteria became much more stringent. If there was no residual paralysis 60 days after onset, the disease was not considered to be paralytic polio. This change made a huge difference in the documented prevalence of paralytic polio because most people who experience paralysis recover prior to 60 days. Dr. Greenberg said:
The change in 1955 meant that we were reporting a new disease, namely, paralytic poliomyelitis with a longer-lasting paralysis. Furthermore, diagnostic procedures have continued to be refined. Coxsackie virus and aseptic meningitis have been distinguished from paralytic poliomyelitis. Prior to 1954 large numbers of these cases were mislabeled as paralytic poliomyelitis. Thus, simply by changes in diagnostic criteria, the number of paralytic cases was predetermined to decrease in 1955-1957, whether or not any vaccine was used.[16]
The Salk vaccine constituted a large-scale medical experiment on the general public. Initial pledges of success were made, but the subsequent failures, injuries, and even fatalities were brushed aside. The individuals responsible were permitted to substitute their hazardous blunders with new ones, and astonishingly, they were lauded by their fellow experimenters and even by the public as reality gave way to a prevailing myth. Victory was declared, yet the new Sabin vaccine quickly replaced the Salk vaccine with shifting case definitions; failures and deaths were all swept under the rug.
Once a live, oral vaccine is fully approved... Because of the doubt about the potency and effectiveness of the Salk vaccine in the past, a full course of the new vaccine will undoubtedly be recommended for everyone, regardless of how many Salk shots each individual has had.[17]
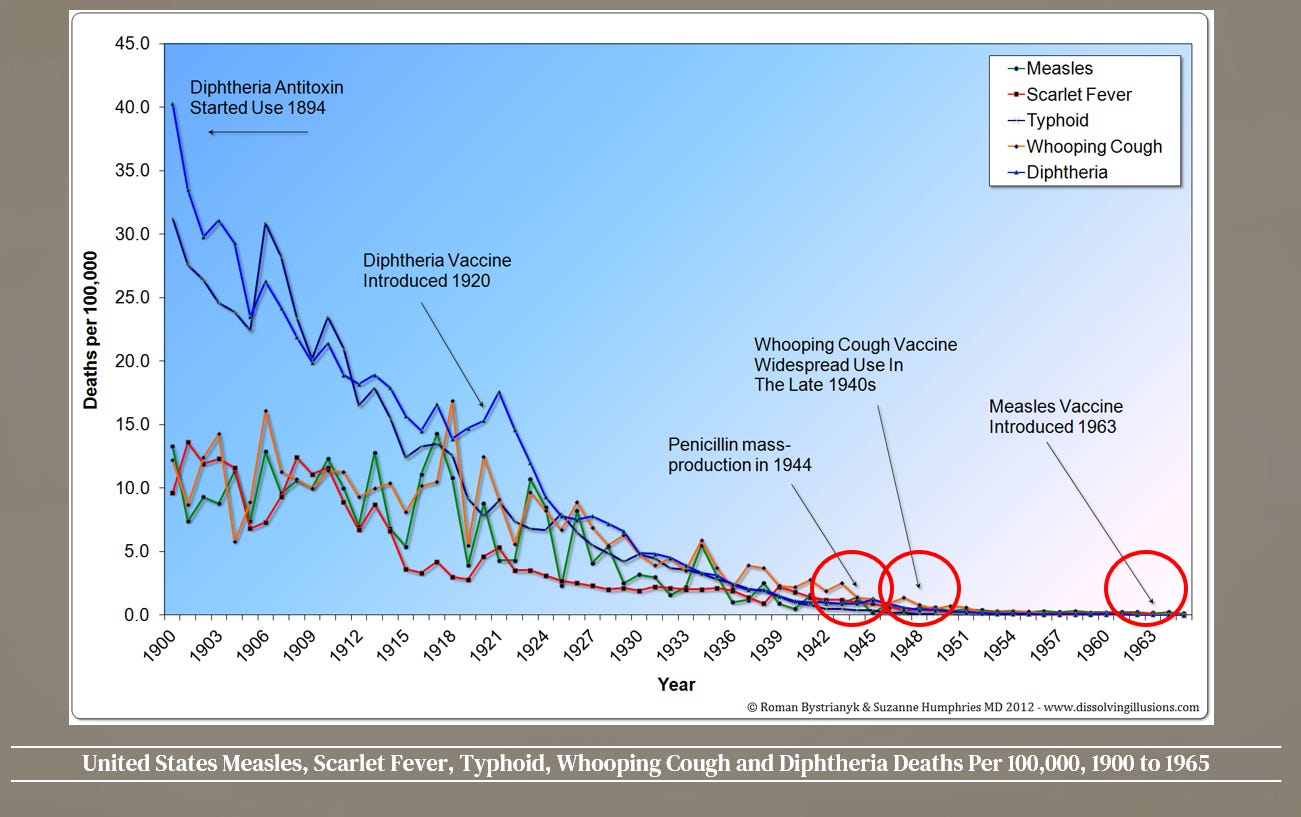
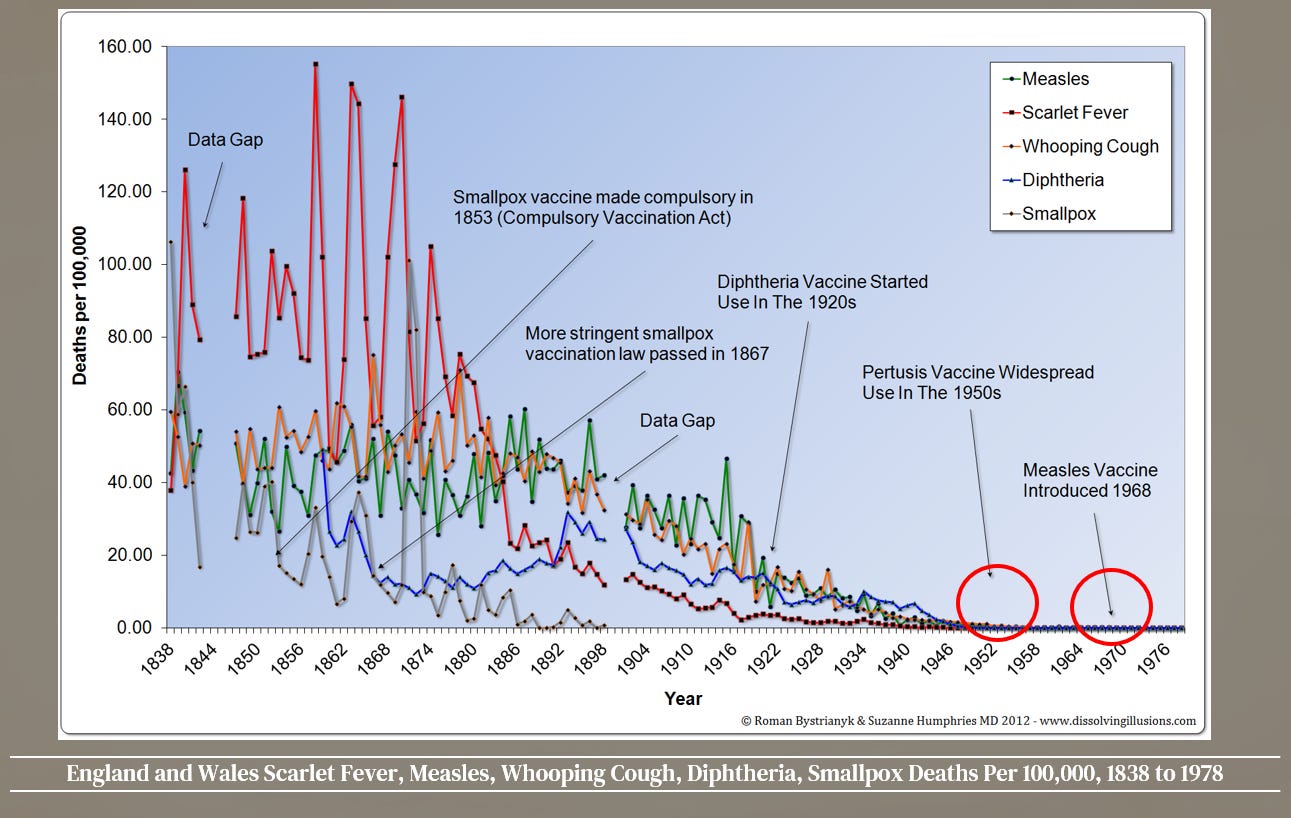
Yet, experimentation and failure didn’t mean you didn’t move forward with the next disease to try and tackle. Even though the death rate had fallen for measles by 98% by 1960, and by nearly 100% if you looked at England and Wales, that didn’t stop the quest for a measles vaccine.
Dr. Langmuir knew that measles was not a disease that needed eradication when he said:
To those who ask me, “Why do you wish to eradicate measles?” I reply with the same answer that Hillary used when asked why he wished to climb Mt. Everest. He said, “Because it is there.” To this may be added, “... and it can be done.”[18]
Langmuir also knew that by the time the vaccine was developed, measles mortality in the United States had already declined to minimal levels when he described measles as a:
...self-limiting infection of short duration, moderate severity, and low fatality...[19]
Despite the greatly diminished danger of measles, news reports in the 1960s urgently called for children to quickly be vaccinated against the disease. Theoretical claims were made that a single shot would provide lifelong immunity.[20]
The United States Public Health Service licensed a new, refined, live-measles vaccine. Although several live vaccines have been licensed since 1963—all of them one-shot treatments that give life immunity without serious side-effects—the new one is considered by epidemiologists as “the best so far in minimizing the side-effects.”[21]
The plan began in 1963 with an expectation of eradication by 1967...
Effective use of these vaccines during the coming winter and spring should ensure the eradication of measles from the United States in 1967.[22]
...if enough of the “right” children were vaccinated.
Measles, the “harmless” childhood disease that can kill, will be nearly eradicated from most areas of the country a year from now, officials of the United States Public Health Service predict... Although there are still more than 12 million susceptible children, vaccination of the “right” two million to four million youngsters could wipe out the disease, according to Dr. Robert J. Warren of the Communicable Disease Center in Atlanta.[23]
The early 1963 measles vaccine that contained the “killed” virus was an aluminum-precipitated vaccine produced from formaldehyde-inactivated monkey kidney cell cultures. A 1967 study revealed that the vaccine could cause pneumonia and encephalopathy (inflammation of the brain).
Pneumonia is a consistent and prominent finding. Fever is severe and persistent and the degree of headache, when present, suggests a central nervous system involvement. Indeed one patient in our series who was examined by EEG, evidence of disturbed electrical activity of the brain was found, suggestive of encephalopathy... These untoward results of inactivated measles virus immunization was unanticipated. The fact that they have occurred should impose a restriction on the use of inactivated measles virus vaccine. We now recommend that inactivated measles virus vaccine should no longer be administered.[24]
In addition to being dangerous, killed vaccines were very ineffective. Whatever vaccine-induced immunity was present declined rapidly, and recipients again became susceptible. They were later advised to be revaccinated with live vaccine in the hope of rectifying the problem. But this approach only led to more problems. Those who were given the live vaccine measles, after having the killed vaccine, had a tendency to develop a more severe disease, atypical measles.
Atypical measles was characterized by a higher and more prolonged fever, unusual skin lesions and severe pneumonitis compared to measles in previously unvaccinated persons. The rash was often accompanied by evidence of hemorrhage or vesiculation. The pneumonitis included distinct nodular parenchymal lesions and hilar adenopathy. Abdominal pain, hepatic dysfunction, headache, eosinophilia, pleural effusions and edema were also described. Cases of atypical measles were reported up to 16 years after receipt of the inactivated vaccine. Administration of the live virus vaccine after 2 to 3 doses of killed vaccine did not eliminate subsequent susceptibility to atypical measles and was often associated with severe reactions at the site of live virus inoculation.[25]
The killed vaccines were quickly abandoned. However, there were also significant issues with the live vaccines, which were not highly attenuated and produced a “modified measles” rash in about half of those injected—essentially equivalent to a case of measles. Forty-eight percent of people had a rash, and 83 percent had fevers up to 106°F post-injection.[26] Even 13 years later, in 1980, atypical measles was still recognized as a serious condition. James D. Cherry wrote in 1980:
“Before turning to my recommendations there is one other point to be addressed: atypical measles. This syndrome was first noted in 1965 but did not receive much attention until 1967, when V. A Fulginiti et al reported a number of cases. It is characterized at first by acute onset of fever, headache, abdominal pain, and myalgia: two to three days later, a yellowish red, maculopapular, and frequently vesicular and petechial skin rash appears, beginning distally and then spreading centrally. In many patients, the extremities are edematous, and pneumonia occurs in almost all (but may not be detected by x-ray). The illness has been described as lasting one to three weeks, but recent reports suggest increasing duration and severity: in 1979, for example. D. B. Martin et al reported persistent residual nodular densities in chest x-rays of patients up to six months after the acute episode of atypical measles.
Although atypical measles has been reported very rarely in patients inoculated with live vaccine only. it usually occurs in recipients of killed vaccine. Since "only" about 1.8 million doses of killed vaccine were distributed between 1963 and 1967, and since "only" an estimated 600,000 to 900,000 children received two or three doses of killed vaccine in those years. it was expected in the early 1970s that the problem would disappear quickly. Eventually (if its pathogenesis involves killed vaccine) it will, but in the meantime, atypical measles is still very much with us. It is a disease of significant morbidity in young adults and some adolescents: it also presents a diagnostic challenge for primary care physicians unfamiliar with exanthematous diseases, particularly those illnesses normally confined to the pediatric population. Moreover, the possibility of misdiagnosis is heightened when the syndrome is incompletely expressed, and the patient's vaccination history is fragmentary, unelicited, or not considered. In the years to come still more cases undoubtedly will occur, and in many the etiology will go unrecognized.”[27]
Despite a death rate that had fallen by close to 100%, whooping cough (or pertussis)was also considered another disease to tackle.
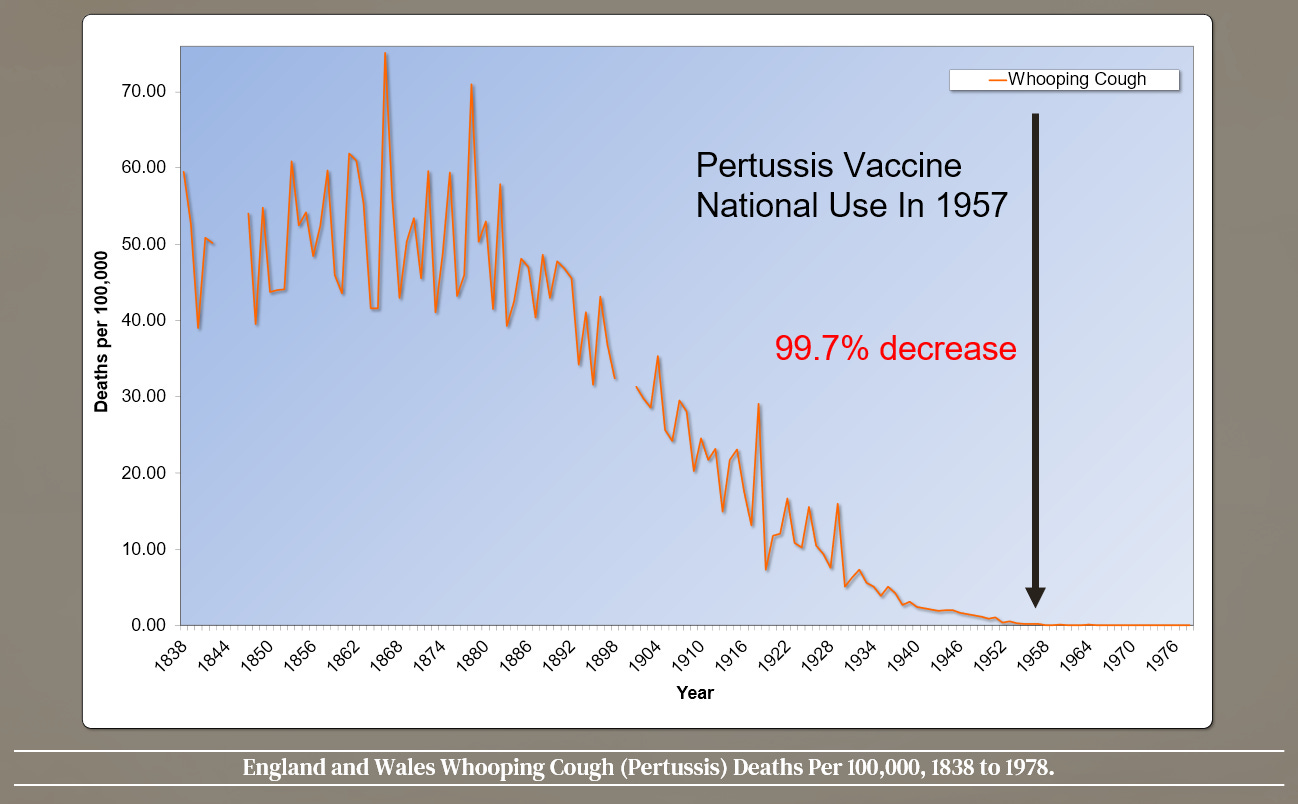
This was despite it becoming a mild disease by the middle to late 1900s, like all other infectious diseases. As noted by Douglas Jenkinson in 1995:
Most cases of whooping cough are relatively mild. Such cases are difficult to diagnose without a high index of suspicion because doctors are unlikely to hear the characteristic cough, which may be the only symptom. Parents can be reassured that a serious outcome is unlikely. Adults also get whooping cough, especially from their children, and get the same symptoms as children.[28]
Yet despite this, the national vaccination of DTP (Diphtheria, Tetanus, Pertussis) began in the United States in the late 1940s and in England by 1957. Very early on, there were indications of problems. A 1946 article discussed twin boys aged 10 months who both died on June 19, 1945, after receiving their second injection of diphtheria and pertussis vaccine.
After the second immunizing injections, both infants cried considerably on reaching home; they vomited and consumed excessive amounts of water, each taking about two full bottles. They then “fell asleep” and when next noticed by their parents appeared “lifeless.”... At 11:30 p. m. when his diaper was changed, he was found to be ice cold and wringing wet with perspiration. The parents explained that they regarded these symptoms as expected effects of the injections and therefore did not summon medical aid until 5:30 a.m., when D. M. appeared to be dead and G. M. gravely ill.[29]
A 1948 article in Pediatrics discussed cases of brain damage following use of the vaccine. The article is hauntingly similar to the large number of cases of autism that would escalate decades later. The children, mostly boys, had been developing normally and showed no problems before receiving the vaccine. They manifested “acute cerebral” symptoms within hours of injection. A regression or “failure of further development” occurred afterward.
Inspection of the records of the Children’s Hospital for the past ten years has disclosed 15 instances in which children developed acute cerebral symptoms within a period of hours after the administration of pertussis vaccine. The children varied between 5 and 18 months in age and, in so far as it is possible to judge children of this age range, were developing normally according to histories supplied by their parents. None had convulsions previously... Twelve of the children were boys and three were girls, a sex difference also encountered in relation to other substances, such as lead, causing gross injury to the developing nervous system. At inoculation time, the children varied in age between 5 and 18 months. Developmental data were obtained in detail on all but two of the children, whose mothers simply stated that they had developed normally. Reference to the case histories showed that such objective activities such as sitting, walking, and talking had appeared in many of the children prior to the inoculations; and the regressions or failure of further development occurred after the encephalopathies [any disease or symptoms of disease referable to disorders of the brain] in several instances. In so far as it was possible to judge none of the children were defective prior to their acute illness.[30]
A 1980 report tied the use of the DTP vaccine to seizures. The author noted that these severe damages were especially abominable because they originated from a medical treatment performed on perfectly healthy children.
...since there is a significant difference between the incidence of spontaneous fits in children of the same age group and the incidence after DTP, a causal relationship between the DTP and the seizures appears to be confirmed... the severe damages are particularly tragic as they are iatrogenic [medically caused] and in most cases affect primarily completely healthy children.[31]
The Institute of Medicine (IOM) was established in 1970 as an independent nonprofit organization that worked outside of government to provide unbiased and authoritative advice to decision-makers and the public. The 1985 IOM report of the U.S. National Academy of Sciences reported on the problem of adverse reactions to the whole-cell pertussis vaccine. The panel estimated that 17,994,600 doses of whole-cell vaccine were given each year. The result was 7,197,840 cases of minor reactions, 10,283 convulsions, 164 cases of encephalitis, and 58 cases of chronic disability, with costs running into the millions. The panel also estimated that the whole-cell DTP caused two to four deaths per year.[32]
As a result of their findings, the IOM recommended a switch to the acellular version, or DTaP, which contained inactivated pertussis toxin (PT) and, depending on the manufacturer, one or more other bacterial components. The hope was that it would greatly reduce the number of reactions by virtue of being a less antigenic substance. Yet the DPT would still be used worldwide, assuming it was acceptable… and cheaper. Again, let’s listen to Stanley Plotkin about DTP in 2018.
Q This is the Peter Aaby study that you and I were talking about earlier, correct?
A This is one of them.Q This is the study in which Peter Aaby found that children who receive DPT in the first six months of life versus those who got no vaccines died at ten times the rate, correct?
A Right.Q And in this study, you earlier said that your concerns with Aaby's prior studies that had similar conclusions was that they weren't randomized; but in this study it was randomized, correct? Because it was -- strike that. In this study, in this study the vaccinated versus unvaccinated children were simply vaccinated or unvaccinated purely by the chance of when their birthday happened to be; isn't that correct?
A Yes. It says they were allocated by birthday. I have to see. Well, you know, it's not absolutely clear as to how the randomization was done. Apparently there were periods of time when they were vaccinating and other periods when they were not vaccinating.Q I think that if you -- have you read this study before, Dr. Plotkin?
A I've glanced at it, yes. I haven't read it thoroughly. But the, as I said before, the, this kind of study is useful. There's no doubt about that. But one needs to have some sort of immunological correlate to really confirm that that, that the findings are real....
A Regardless, my point is that mortality in the developed world is relatively rare in childhood; whereas, in Africa it's obviously common. Let me repeat what I said about Peter Aaby's work. It's not that I discard it or think that his conclusions are wrong. What I'm saying is that they are observational data, and they have to be confirmed by studies of the immune responses. And those have been done only to a certain degree.
...
Q So what you're saying is you don't dispute his findings that at least in this African country --
A Yes.Q -- there is a ten-times-greater death rate amongst those who got DPT -- TP in the first six months of life versus those who got no vaccines, correct?
A I don't dispute his findings. I would have to look further to make sure that the populations that were studied were absolutely equal in other respects.Q Okay.
A But, again, I'm not one who discards Peter's studies a priori.Q Earlier you told me the issue was it wasn't randomized, but now --
A That is an important issue, yes.Q And it is, this one is randomized?
A Well, again, I just have to be sure that it was randomized, that both groups were vaccinated or non-vaccinated at the same time rather than sequentially.Q Yes. Because it was done by birthdays. When people came into the clinics, right, depending on their birth date, they either got the vaccine or they didn't, correct?
A Well, subject to my reading this carefully, I agree that he is claiming that it's randomized.Q So DTaP has been used around the world for what, 30, 40 years now, 50 years?
A Mainly since the 1990s.Q Okay. Mainly since the 1990s.
A So about 20 years.Q And Peter Aaby has been claiming, making this claim, a respected scientist whose conclusions you said you take seriously, that DTP might cause more deaths than people it saves --
A Yeah, I --Q -- but -- let me just finish my question, please. When do you think this extra science on immunology you think is necessary is going to get done so we know whether or not DTP is saving more children than it kills?
A Well, I would imagine that WHO is looking into it. I don't know that for a fact. But it also has to be pointed out that the vaccine that he's studying is whole-cell vaccine; it is not the vaccine being used in the United States.Q That's right. But it is being used in most third-world countries, correct?
A In, the vaccines being used in the United States are being used in the U.S. and Europe.Q The DTP --
A But the DTP, the whole-cell vaccine is used very largely in Latin America and Africa.Q In developing countries?
A Yes.Q Any reason that the life of a child in a developing country is not equal to that in the first-world country?
A No.Q Okay.
A But the whole-cell vaccine is considerably cheaper.
“A ten-times-greater death rate amongst those who got DTP in the first six months of life versus those who got no vaccines,” Plotkin says, “I don't dispute his findings, and I would imagine that WHO is looking into it.” It is simply shocking that there isn’t a call to action to investigate this possible devastating disaster.
The same Aaby discussed in the case by Plotkin stated in 2017 that:
It should be of concern that the effect of routine vaccinations on all-cause mortality was not tested in randomized trials. All currently available evidence suggests that DTP vaccine may kill more children from other causes than it saves from diphtheria, tetanus, or pertussis. Though a vaccine protects children against the target disease it may simultaneously increase susceptibility to unrelated infections.[33]
It is disturbing, to say the least, that the DTP vaccine that was replaced with a safer DTaP wasn’t done for the poor of the world for it seems profit reasons. But that’s not all. A 2005 article[34] on pertussis had a telling introduction:
The diagnosis of pertussis is frequently missed, often because of misconceptions that whooping cough is solely a pediatric illness that has been controlled by routine childhood immunizations and that immunity resulting from pertussis disease or immunization is lifelong.
Misconception? Another experiment gone awry? The only problem with that statement is the assumption that natural immunity is not lifelong. Before the pertussis vaccine was introduced, lengthy natural immunity was, in fact, the norm because of the natural family and community dynamics. In the 1940s, pertussis was considered only a childhood illness. If an adolescent or adult got it, everyone was astonished.
A diagram from the same article shows that only children had a clinical episode of pertussis, and generational family interactions ensured that those naturally immune from infection retained their immunity due to regular exposure to the younger generations being infected.
Vaccination turned that on its head because vaccinologists were ignorant about the immunological pathways that result in solid, durable, real herd immunity, as opposed to the fake hijacked idea of vaccine herd immunity. The ignorance of the past has brought us to the position we are in now, which is illustrated in the figure.
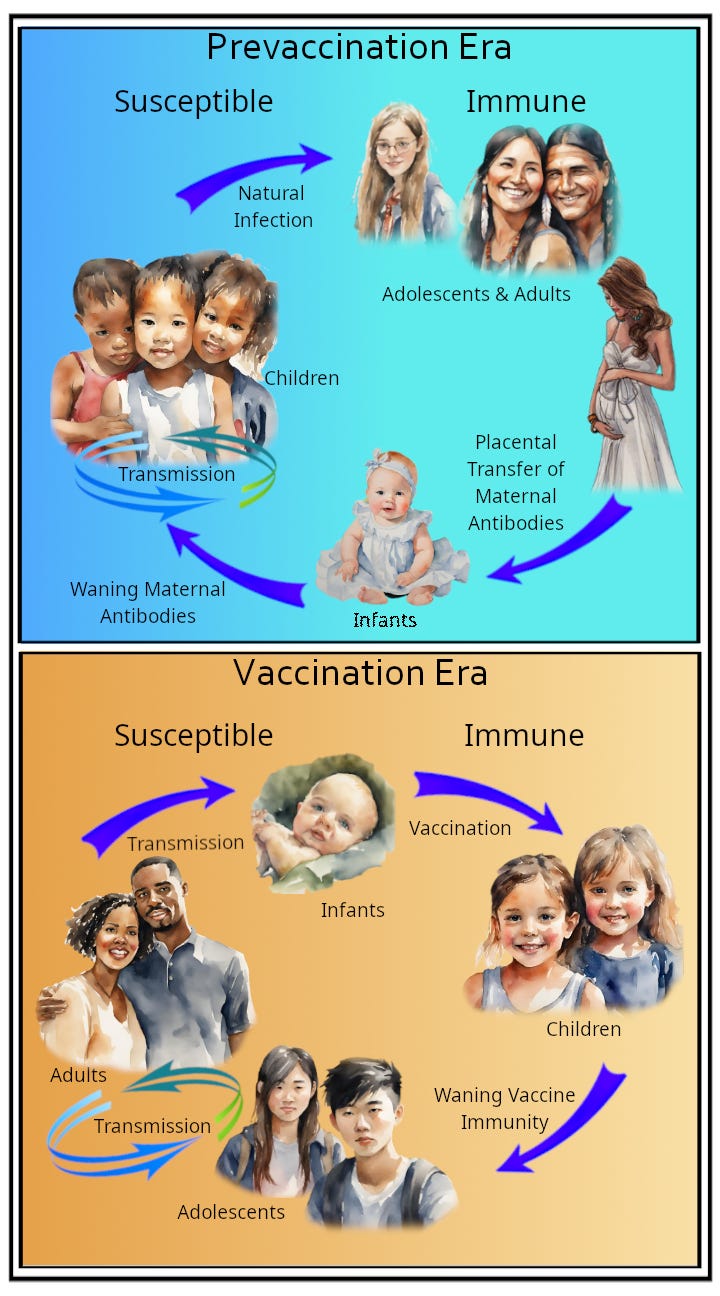
Instead of being a predominantly childhood disease, pertussis now affects adolescents and adults. Worse still, infants that once had strong maternal antibodies are now vulnerable. The pertussis vaccinations have totally changed the face of pertussis epidemiology; they have wrecked how people became immune in the first place, resulting in the vaccinated becoming walking laboratories, colonized with pertussis bacteria that mutate into new strains.
That process started in the 1950s due to the use of the whole cell vaccine, then accelerated once the less effective but “safer” acellular vaccine (DTaP) resulted in longer airway colonization upon re-exposure to pertussis bacteria. But the problems of this new experiment would soon be shown.
For nonscientific reasons, currently licensed aP [acellular pertussis] vaccines include chemically detoxified PT [pertussis toxin]. Chemical detoxification, however, means protein denaturation and thus potential alterations of the tridimensional structure... this denaturation process indeed generates distinct epitopes from the ones present in naïve PT.[35]
The article goes on to describe that the resulting vaccine antibodies would be “vaccine antigen specific.” An antibody is shape specific. Imagine a door lock: the inside of a lock has a unique shape and needs a key cut specifically to fit the shape of the lock. The vaccine toxin was so distorted by the chemical preparation that the vaccine-induced antibody, which matches the vaccine toxin, can’t match and attach to the very differently shaped wild bacterial toxins.
The authors also point out that whooping cough infection is strictly a mucosal pathogen with no bacteria accessing the blood compartment. The local immune systems in the airways have specialized programs to limit the migration of antigen-loaded dendritic cells to the lymph nodes. Yet injected acellular pertussis vaccines do not even engage with this crucial part of immune development.
Another team led by Burdin, with Stanley Plotkin as a co-author, published in the same journal[36] on the same topic and made the observation that the T-cell profile induced by the aP vaccine “is inefficient at conferring protection against colonization and hence transmission, and this induction of a different T-cell response may be crucial to more prolonged protection.”
They went on to point out that the ability of the whole-cell pertussis vaccine to block transmission was also up for debate, as “The Fine and Clarkson (1982) study failed to show prevention of transmission,” something confirmed by a Warfel[37] baboon study, which showed that recipients of the whole-cell vaccine were colonized for two weeks on re-exposure to pertussis.
Veteran pertussis guru James D. Cherry commented on this problem in an article with a shocking title: “The 112-Year Odyssey of Pertussis and Pertussis Vaccines—Mistakes Made and Implications for the Future.”
Because of linked-epitope suppression, all children who were primed by DTaP vaccines will be more susceptible to pertussis throughout their lifetimes, and there is no easy way to decrease this increased lifetime susceptibility.[38]
There is, of course, a lot more—a whole lot more—to all this that you can research and learn about. Unlike most in the government and medical system, I think you should do your own research and understand what goes into your body, not simply dictate what you must do and then attack and punish those who disagree. That’s what freedom means – the right to learn and choose. The other is just despotism.
Do you feel betrayed and violated? Do you think governments and the medical profession have your best interests at heart? Do you feel you’ve been given all the information to make an appropriate decision about… well, anything? Fear not, fellow lab rats at least now you know more than before, so you can now do more research and possibly make different and better decisions. The more distressing question—if that’s possible—is what other experiments are going on right now that you don’t know about to the unsuspecting lab rats?
The inutility and danger of the popular practice of medicine,—which, not being founded on any fixed principles of science, is purely experimental and conjectural, consisting in administering thousands of different drugs, and ten thousand times ten thousand different combinations of drugs, and with as many diversified intentions, and, consequently, of hurrying multitudes to premature graves.[39]
— Charles Rooke, MD, author of Anti-lancet, Or, The Destructive Practice of Bleeding, &c., Exposed and Denounced; Showing the Principles of Life and Death, and the Origin of All Diseases, 1862
[1] “Medical Opinion on Vaccination,” Journal of Hygeio-therapy, vol. II, no. 2, February 1888, pp. 34–35.
[2] https://www.medicalnewstoday.com/articles/how-the-thalidomide-scandal-led-to-safer-drugs
[3] https://www.newscientist.com/article/dn6918-up-to-140000-heart-attacks-linked-to-vioxx
[4] https://www.latimes.com/archives/la-xpm-2000-jun-04-mn-37375-story.html
[5] https://www.cbsnews.com/news/diabetes-drug-and-risk-avandia-linked-to-stroke-heart-trouble-deaths
[6] https://trialsjournal.biomedcentral.com/articles/10.1186/cvm-2-5-205
[7] Robert B. Talley, MD and Marc F. Laventurier, PharmB, “Drug-Induced Illness,” Journal of the American Medical Association, August 19, 1974, https://jamanetwork.com/journals/jama/article-abstract/356271
[8] Jeffery A. Johnson and Lyle Bootman, “Drug-related morbidity and mortality. A cost-of-illness model,” Journal of Managed Care Pharmacy, Jan/Feb 1996, vol. 2, no. 1, pp. 39-47, https://www.jmcp.org/doi/pdf/10.18553/jmcp.1996.2.1.39
[9] Donald W. Light, Joel Lexchin, and Jonathan J. Darrow, “Institutional Corruption of Pharmaceuticals and the Myth of Safe and Effective Drugs,” The Journal of Law, Medicine & Ethics, October 2013, vol. 41, issue 3, https://journals.sagepub.com/doi/10.1111/jlme.12068
[10] James, John T. PhD, “A New, Evidence-based Estimate of Patient Harms Associated with Hospital Care,” Journal of Patient Safety, September 2013, pp. 122-128, https://journals.lww.com/journalpatientsafety/Fulltext/2013/09000/A_New,_Evidence_based_Estimate_of_Patient_Harms.2.aspx
[11] Professor Martin A Makary, "Medical error—the third leading cause of death in the US," British Medical Journal, May 2016,
https://www.hcp.med.harvard.edu/sites/default/files/methodsmakarydaniel_2016_bmj%20%281%29.pdf
[12] https://archive.org/details/2015-831539-DM; https://www.lumenfidei.ie/documents/dr-stanley-plotkin-testimony.pdf
[13] Joan Beck, “The Truth About the Polio Vaccines,” Chicago Sunday Tribune, March 5th, 1961.
[14] Joan Beck, “The Truth About the Polio Vaccines,” Chicago Sunday Tribune, March 5th, 1961.
[15] Paul Offit, MD, The Cutter Incident, 2005, Yale University Press, p. 89.
[16] H. Ratner et al., “The Present Status of Polio Vaccines,” Illinois Medical Journal, vol. 118, nos. 2, 3, pp. 84–93,160–68. Edited from a transcript of a panel discussion presented before the Section on Preventive Medicine and Public Health at the 120th annual meeting of the Illinois State Medical Society in Chicago, May 26, 1969.
[17] Joan Beck, “The Truth About the Polio Vaccines,” Chicago Sunday Tribune, March 5th, 1961.
[18] A. Langmuir, “The Importance of Measles as a Health Problem,” American Journal of Public Health, vol. 52, no. 2, 1962, pp. 1–4.
[19] Ibid.
[20] The Medical Officer, vol. 118, 1967, p. 79.
[21] “Thaler to Hold State Senate Hearing to Find Fastest Way to Expedite Plan,” New York Times, February 24, 1965.
[22] David J. Sencer, MD; H. Bruce Dull, MD; and Alexander D. Langmuir, MD, “Epidemiologic Basis for Eradication of Measles in 1967,” Public Health Reports, vol. 82, no. 3, March 1967, p. 256.
[23] Jane E. Brody, “Measles Will Be Nearly Ended by ’67, U.S. Health Aides Say,” New York Times, May 24, 1966.
[24] Vincent A. Fulginiti, MD; Jerry J. Eller, MD; Allan W. Downie, MD; and C. Henry Kempe, MD, “Altered Reactivity to Measles Virus: Atypical Measles in Children Previously Immunized with Inactivated Measles Virus Vaccines,” Journal of the American Medical Association, vol. 202, no. 12, December 18, 1967, p. 1080.
[25] D. Griffin et al., “Measles Vaccines,” Frontiers in Bioscience, vol. 13, January 2008, pp. 1352–1370.
[26] “Measles Vaccine Effective in Test—Injections with Live Virus Protect 100 Per Cent of Children in Epidemics,” New York Times, September 14, 1961.
[27] James D. Cherry, The 'New' Epidemiology of Measles· and Rubella, Hospital Practice, July 1980, p. 53.
[28] Douglas Jenkinson, “Natural Course of 500 Consecutive Cases of Whooping Cough: A General Practice Population Study,” British Medical Journal, vol. 310, February 1995, p. 299.
[29] Jacob Werne, MD, and Irene Garrow, MD, “Fatal Anaphylactic Shock: Occurrence in Identical Twins Following Second Injection of Diphtheria Toxoid and Pertussis Antigen,” Journal of the American Medical Association, vol. 131, no. 9, June 1946, pp. 731–732.
[30] Randolph K. Byers, MD, and Frederic C. Moll, MD, “Encephalopathies Following Prophylactic Pertussis Vaccine,” Pediatrics, vol. 1, no. 4, April 1948, pp. 438–439, 443.
[31] O Tönz and S. Bajc, “Convulsions After Pertussis Vaccination,” Schwiez Med Wochenschr, vol. 110, December 20, 1980, p. 13.
[32] New Vaccine Development Establishing Priorities, Volume I, Diseases of Importance in the United States, Part One of a Two-Part Study by the Committee on Issues and Priorities for New Vaccine Development Division of Health Promotion and Disease Prevention, Institute of Medicine, National Academy Press, Washington, D.C., 1985, pp. 172–173, 175.
[33] Mogensen SW, Andersen A, Rodrigues A, Benn CS, Aaby P., “The Introduction of Diphtheria-Tetanus-Pertussis and Oral Polio Vaccine Among Young Infants in an Urban African Community: A Natural Experiment,” EBioMedicine. 2017 Mar;17:192-198. doi: 10.1016/j.ebiom.2017.01.041. Epub 2017 Feb 1. PMID: 28188123; PMCID: PMC5360569, accessed February 15, 2024
[34] Erik L Hewlett and Kathryn M Edward, “Clinical practice. Pertussis—not just for kids,” New England Journal of Medicine, March 24, 2005 (12), pp. 1215–1222., doi: 10.1056/NEJMcp041025, PMID: 15788498, accessed February 14, 2024
[35] Eberhardt CS, Siegrist CA, “What Is Wrong with Pertussis Vaccine Immunity? Inducing and Recalling Vaccine-Specific Immunity,” Cold Spring Harbor Perspectives in Biology, 2017 Dec 1;9(12): a029629. doi: 10.1101/cshperspect.a029629. PMID: 28289058; PMCID: PMC5710108, accessed February 15, 2024.
[36] Nicolas Burdin, Lori Kestenbaum Handy, Stanley A Plotkin, “What is wrong with Pertussis vaccine immunity? The problem of waning effectiveness of Pertussis vaccines,” Cold Spring Harbor Perspectives in Biology, December 1, 2017, vol. 9, issue 12.
[37] Jason M. Warfel, Lindsey I. Zimmerman, and Tod J. Merkel, “Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model,” Proceedings of the National Academy of Sciences, 2013.
[38] J. D. Cherry, MD, “The 112-Year Odyssey of Pertussis and Pertussis Vaccines—Mistakes Made and Implications for the Future,” Journal of the Paediatric Infectious Diseases Society, September 2019, pp. 334–341.
[39] Charles Rooke, MD, Anti-lancet, Or, The Destructive Practice of Bleeding, &c., Exposed and Denounced; Showing the Principles of Life and Death, and the Origin of All Diseases, 1862, Printer for the Author by J. Hammer, 7 Briggate, Leeds, pp. 26–27.